
Մասնակից:Eema97/Ավազարկղ
Լյարդաբջջային քաղցկեղ (ԼԲՔ) մեծահասակների մոտ լյարդի առաջնային քաղցկեղի ամենատարածված տեսակն է և ներկայումս ցիռոզով հիվանդ մարդկանց մահվան ամենատարածված պատճառն է[1]։ ԼԲՔ-ն աշխարհում քաղցկեղից մահացության երրորդ առաջատար պատճառն է[2]։
IԼյարդաբջջային կարցինոման առաջանում է լյարդի քրոնիկ բորբոքման պայմաններում և սերտորեն կապված է քրոնիկական վիրուսային հեպատիտի (հեպատիտ B կամ C) կամ տոքսինների ազդեցության հետ, ինչպիսիք են ալկոհոլը, աֆլատոքսինը կամ պիրոլիզիդին ալկալոիդները: Որոշ հիվանդություններ, ինչպիսիք են հեմոքրոմատոզը և ալֆա 1-անտիտրիպսինի անբավարարությունը, զգալիորեն մեծացնում են ԼԲՔ-ի զարգացման ռիսկը: Մետաբոլիկ համախտանիշը և ոչ ստերոիդային հակաբորբոքային դեղամիջոցները նույնպես համարվում են ԼԲՔ-ի ռիսկի գործոններ[3]։
Ինչպես ցանկացած քաղցկեղի դեպքում, ԼԲՔ-ի բուժումը և կանխատեսումը ևս կախված է ուռուցքի հիստոլոգիական առանձնահատկություններից, չափից, քաղցկեղի տարածվածությունից և հիվանդի ընդհանուր առողջական վիճակից:
Լյարդաբջջային քաղցկեղի դեպքերի ճնշող մեծամասնությունը և բուժումից հետո ապրելիության ամենացածր ցուցանիշները գրանցվում են Ասիայում և Ենթասահարյան Աֆրիկայում, այն երկրներում, որտեղ հեպատիտ B-ն համարվում է էնդեմիկ վարակ, և շատերը մոտ վարակումը բնածին է: ԱՄՆ-ում և այլ զարգացող երկրներում ԼԲՔ-ով հիվանդացությունը աճում է հեպատիտ C վիրուսով վարակվածության աճի հետևանքով: Տղամարդկանց մոտ անհայտ պատճառներով հիվանդացությունը ավելի քան չորս անգամ հաճախ է, քան կանանց մոտ[3]։
Նշաններ և ախտանիշներ[խմբագրել | խմբագրել կոդը]
ԼԲՔ-ի դեպքերի մեծ մասը հանդիպում է այն մարդկանց մոտ, ովքեր արդեն ունեն լյարդի քրոնիկ հիվանդության նշաններ և ախտանիշներ: Դրանք կարող են դրսևորվել ախտանիշներրի վատթարացումով կամ ախտանիշները կարող են բացակայել: ԼԲՔ-ը կարող է դրսևորվել ոչ սպեցիֆիկ ախտանիշներով, ինչպիսիք են որովայնի ցավը, սրտխառնոցը, փսխումը կամ հոգնածության զգացումը: Որոշ ախտանշաններ, որոնք ավելի սերտերեն են կապված լյարդի հիվանդությունների հետ, ներառում են դեղնուկը (դեղնախտ), որովայնի մեծացում՝ որովայնի խոռոչում առկա հեղուկի պատճառով, կապտուկներ՝ պայմանավորված արյան մակարդման խանգարումներից հետ , ախորժակի կորուստ, քաշի կորուստ, որովայնի ցավ, սրտխառնոց, փսխում կամ հոգնածության զգացում[4]։
Ռիսկի գործոններ[խմբագրել | խմբագրել կոդը]
Քանի որ ԼԲՔ-ն հիմնականում առաջանում է լյարդի ցիռոզով հիվանդ մարդկանց մոտ, ռիսկի գործոնները հիմնականում այն գործոններ են, որոնք առաջացնում են լյարդի քրոնիկ հիվանդություններ, որոնք էլ իրենց հերթին կարող են հանգեցնել լլարդի ցիռոզի առաջացման: Այնուամենայնիվ, ռիսկ որոշ գործոններ ավելի շատ են կապված ԼԲՔ-ի հետ, քան մյուսները: Օրինակ, ալկոհոլի չարաշահումը գնահատվում է որպես ցիռոզի 60-70%-ի պատճառ, ԼԲՔ-ի ճնշող մեծամասնությունը առաջանում է վիրուսային հեպատիտի հետևանքով առաջացած ցիռոտիկ լյարդում[5]։
Ճանաչված ռիսկի գործոններն են՝
- Քրոնիկ վիրուսային հեպատիտ (ընդհանուր դեպքերի 80% )
- Տոքսիններ՝
- Լյարդի ալկոհոլային հիվանդություն [5]
- Աֆլատոքսին
- Հեմոքրոմատոզ
- Պիրոլիզիդին ալկալոիդները
- Մետաբոլիկ՝
- Ոչ ալկոհոլային ստեատոհեպատիտ (20% պրոգրոսիա դեպի ցիռոզ)[7]
- լյարդի ոչ ալկոհոլային ճարպային հիվանդություն[8]
- Տիպ 2 շաքարային դիաբետ (հավանակ կապված ճարպակալման հետ)[9]
- Բնածին խանգարումներ
- Ալֆա 1-անտիտրիպսինի անբավարարությունը
- Վիլսոնի հիվանդություն (Հակասական; ոմանք կարծում են, որ ռիսկը մեծանում է,[10] Մինչդեռ դեպքերի ուսումնասիրությունները հազվադեպ են [11] և վկայում են հակառակը, որ Վիլսոնի հիվանդությունը իրականում կարող է պաշտպանել[12]։)
- Հեմոֆիլիա, although statistically associated with higher risk of HCC,[13] this is due to coincident chronic viral hepatitis infection related to repeated blood transfusions over lifetime.[14]
Այս ռիսկի գործոնների նշանակությունը տարբեր է: Այն տարածաշրջաններում, որտեղ հեպատիտ B-ն էնդեմիկ է, օրինակ՝ հարավ-արևելյան Չինաստանը, հեպատիտ B-ն լյարդի ցիռոզի գերակշռող պատճառն է[15]։Հեպատիտ B-ի դեմ պատվաստումներով պաշտպանված պոպուլյացիաներում, ինչպիսիք են Միացյալ Նահանգները, ԼԲՔ-ն առավելապես կապված է այնպիսի ցիռոզի պատճառների հետ, ինչպիսիք են քրոնիկ հեպատիտ C-ն, գիրությունը և ալկոհոլի չափից ավելի օգտագործումը[16]։
Լյարդի որոշ բարորակ ուռուցքներ, ինչպիսիք են լյարդաբջջային ադենոման, երբեմն կարող են կապված լինել չարորակ ԼԲՔ-ի հետ: Բարորակ ադենոմաների հետ չաորորակացման դեպքերի հետ կապված ապացույցները սահմանափակ են. Այնուամենայնիվ, համարվում է, որ լյարդի ադենոմայի չափը կապված է չարորակացման ռիսկի հետ, ուստի մեծ ուռուցքները կարող են հեռացվել վիրահատական ճանապարհով: Ադենոմայի որոշ ենթատեսակներ, մասնավորապես β-CAM ենթատեսակ ունեցողները, ունեն ԼԲՔ-ի բարձր ռիսկի[16]։
Երեխաների և դեռահասների մոտ լյարդի քրոնիկ հիվանդությունները հազվադեպ են. Այնուամենայնիվ, լյարդի բնածին խանգարումները կապված են ԼԲՔ-ի զարգացման հավանականության մեծացման հետ[17]։ Մասնավորապես, լեղուղիների ատրեզիայով, մանկական խոլեստազով, գլիկոգեն-պահեստավորման հիվանդություններով և լյարդի այլ ցիռոտիկ հիվանդություններ ունեցող երեխաները մանկության հասակում հակված են ԼԲՔ-ի զարգացմանը։
Երիտասարդ մեծահասակները, որոնք տառապում են լյարդաբջջային քաղցկեղի հազվագյուտ ֆիբրոլամելյար տարբերակով, կարող են բնորոշ ռիսկի գործոններից ( ցիռոզը և հեպատիտը ) ոչ մեկը չունենալ[16]:
Շաքարային դիաբետ[խմբագրել | խմբագրել կոդը]
Տիպ 2 դիաբետով հիվանդների մոտ հեպատոցելուլյար քաղցկեղի վտանգը ավելի մեծ է (2,5-ից[9]մինչև 7,1[18] անգամ)՝ կախված շաքարախտի տևողությունից և բուժումից: Այս ռիսկի գործոնի կասկածելի աճը կապված է շրջանառվող ինսուլինի կոնցենտրացիայի հետ։ Շաքարախտով այն հիվանդները, որոնք ունեն ինսուլինի մակարդակի վատ վերահսկում կամ բուժուման արդյունքում ինսուլինի արտադրության բարձրացում (երկու վիճակներն էլ նպաստում են շրջանառվող ինսուլինի կոնցենտրացիայի բարձրացմանը), ունեն լյարդաբջջային քաղցկեղի զարգացման ավելի մեծ ռիսկ, քան շաքարախտով այն հիվանդները, որոնց բուժումը նվազեցնում է շրջանառվող ինսուլինի կոնցենտրացիան[9][18][19][20]։ Այս նկատառումով, որոշ դիաբետիկներ, ովքեր զբաղվում են ինսուլինի խիստ վերահսկողությամբ (հսկելով մակարդակի բարձրացումը), ռիսկի մակարդակը բավական ցածր է, և չի տարբերվում ընդհանուր բնակչության ռիսկի գործոնից[18][19]։Այսպիսով, այս երևույթը միայն 2-րդ տիպի շաքարային դիաբետի հետ չի կապված, քանի որ ինսուլինի վատ կարգավորումը հայտնաբերվում է նաև այլ դեպքերում, ինչպիսիք են մետաբոլիկ համախտանիշը (մասնավորապես, երբ առկա են լյարդի ոչ ալկոհոլային ճարպային հիվանդություն)[21][22]։ Կան պնդումներ, որ անաբոլիկ ստերոիդներ չարաշահողները ավելի մեծ ռսիկ ունեն[23] (ենթադրվում է, որ դա պայմանավորված է ինսուլինի և աճի ինսուլինանաման գործոն հետ[24][25]), սակայն միակ ապացույցը, որը հաստատել է այս պնդումը կապված է անաբոլիկների ազդեցությամբ ադենոմաների չարորակացման վտանգի հետ[26][27]։
Պաթոգենեզ[խմբագրել | խմբագրել կոդը]
Հեպատոցելուլյար քաղցկեղը, ինչպես ցանկացած այլ քաղցկեղ, զարգանում է, երբ բջջային մեխանիզմների վրա ազդող էպիգենետիկ փոփոխությունները և մուտացիաները, առաջացնում են բջիջների ռեպլիկացիայի հաճախության բարձրացում և/կամ հանգեցնում են բջիջների ապոպտոզից խուսափելուն[28]։
Մասնավորապես, քրոնիկ հեպատիտ B և/կամ C վարակները կարող են նպաստել լյարդաբջջային քաղցկեղի զարգացմանը՝ բրելով մարմնի սեփական իմունային համակարգի կողմից լյարդի բջիջների վրա հարձակումների, որոնցից միայն մի մասն են վարակված են վիրուսով, իսկ մյուսները՝ ոչ[29]։ Ակտիվացված իմունային համակարգի բորբոքային բջիջների կողմից արտադրվում են ազատ ռադիկալներ, ինչպիսիք են թթվածնի ռեակտիվ տեսակները և ազոտի օքսիդի ռեակտիվ տեսակները։ Այս ազատ ռադիկալները իրենց հերթին կարող են առաջացնում են ԴՆԹ-ի վնասում և հանգեցնում են քաղցկեղածին գենային մուտացիաների[30]։ Թթվածնի ազատ ռադիկալները նաև առաջացնում են ԴՆԹ-ի ռեպլիկացիայի էպիգենետիկ փոփոխություններ[31]։
Վնասման այս հաստատուն ցիկլը, որին հաջորդում է վերականգնումը, վերականգման ընթացքում կարող է հանգեցնել սխալների, որոնք իրենց հերթին հանգեցնում են քաղցկեղի առաջացման։ Այս վարկածը ներկայումս ավելի կիրառելի է հեպատիտ C-ի համար: Քրոնիկ հեպատիտ C-ն առաջացնում է ԼԲՔ ցիռոզի փուլով: Քրոնիկ հեպատիտ B-ի դեպքում վիրուսային գենոմի ինտեգրումը վարակված բջիջ կարող է ուղղակիորեն բերել ոչ ցիռոտիկ ԼԲՔ զարգացման: Որպես այլընտրանք, մեծ քանակությամբ էթանոլի շարունակական օգտագործումը կարող է նմանատիպ ազդեցություն ունենալ: Ասպերգիլուս սնկերի որոշ տեսակների թույն աֆլատոքսինը քաղցկեղածին է և կուտակվելով լյարդում նպաստում է լյարդաբջջային քաղցկեղի առաջացմանը: Աֆլատոքսինի և հեպատիտ B-ի համակցված բարձր տարածվածությունը այնպիսի վայրերում, ինչպիսիք են Չինաստանը և Արևմտյան Աֆրիկան, հանգեցրել է լյարդաբջջային քաղցկեղի հիվանդացության համեմատաբար բարձր ցուցանիշների: Այլ վիրուսային հեպատիտներ, ինչպիսիք են հեպատիտ A-ն, չունեն քրոնիկ վարակ դառնալու պոտենցիալ, հետևաբար կապված չեն ԼԲՔ-ի հետ[16]։
Ախտորոշում[խմբագրել | խմբագրել կոդը]
Լյարդաբջջային քաղցկեղիի ախտորոշումը բժշկական պատկերավորման բարելավմամբ հետ կապված զզարգացել է: Ինչպես ասիմպտոմատիկ հիվանդների, այնպես էլ լյարդային հիվանդության ախտանիշ ունեցող հիվանդների գնահատումը ներառում է արյան քննության և գործիքային մեթոդների արդյունքների գնահատում: Պատմականորեն, ԼԲՔ-ի հստակ ախտորոշման համար անհրաժեշտ էր ուռուցքի բիոպսիա: Այնուամենայնիվ, վիզուալիազացիայի մեթոդները (հատկապես ՄՌՏ) կարող են բավական համոզիչ լինել[16]։
Սկրինինգ[խմբագրել | խմբագրել կոդը]
ԼԲՔ-ը շարունակում է կապված լինել մահացության բարձր մակարդակի հետ, մասամբ այն պատճառով, որ նախնական ախտորոշումը սովորաբար կատարվում է հիվանդության ուշ փուլում: Ինչպես քաղցկեղի այլ տեսակների դեպքում, արդյունքները զգալիորեն բարելավվում են, եթե բուժումը սկսվում է հիվանդության ավելի վաղ փուլերում: Քանի որ ԼԲՔ-ի դեպքերի ճնշող մեծամասնությունը առաջանում է լյարդի որոշ քրոնիկ հիվանդություններ ունեցող մարդկանց մոտ, հատկապես ցիռոզով հիվանդների մոտ, հետևաբար լյարդի սկրինինգը սովորաբար առաջարկվում է կատարել այս պոպուլյացիաում։ Ժժամանակի ընթացքում կրինինգի հատուկ ուղեցույցները շարունակում են զարգանալ։Լյարդի հիվանդությունների ուսումնասիրման ամերիկյան ասոցիացիայի (AASLD) կողմից հրապարակված ուղեցույցները խորհուրդ են տալիս ցիռոզով հիվանդ մարդկանց յուրաքանչյուր վեց ամիսը մեկ կատարել ուլտրաձայնային հետազոտություն՝ արյան մեջ ուռուցքային մարկեր ալֆա-ֆետոպրոտեինի մակարդակի չափմամբ կամ առանց դրա:[32]
ԱՖՊ-ի բարձր մակարդակները կապված են ակտիվ ԼԲՔ հիվանդության հետ, թեև դրանց հուսալիությունը կարող է անհամապատասխան լինել ( >20 ), զգայունությունը 41–65% է, իսկ սպեցիֆիկությունը՝ 80–94%։ Այնուամենայնիվ, 200-ից բարձր մակարդակի դեպքում զգայունությունը 31 է, իսկ սպեցիֆիկությունը՝ 99%[33]։
Ուլտրաձայնային հետազոտության ժամանակ ԼԲՔ-ը հաճախ դիտվում է որպես վատ սահմանագծված եզրերով, կոպիտ, անկանոն ներքին ներառուկներով, փոքր հիպոէխոգեն ախտահարում: Ուռուցքի մեծաման հետ զուգահեռ կարող է դիտվել տարասեռություն կապված ֆիբրոզի, ճարպային փոփոխությունների և կալցիֆիկացիաների առկայության հետ: Այս տարասեռությունը կարող է նման լինել ցիռոզին և շրջակա լյարդի պարենքիմային: ՈՒՁՀ զգայունությունը կազմում է 60% (95% CI 44–76%), իսկ սպեցիֆիկությունը՝ 97% (95% CI 95–98%)[34]։
Բարձր ռիսկ ունեցողներ[խմբագրել | խմբագրել կոդը]
Այն անձինք, ովքեր ունեն ԼԲՔ-ի առկայության բարձր կասկած, օրինակ՝ ախտանիշներով կամ արյան աննորմալ թեստերով (այսինքն՝ ալֆա-ֆետոպրոտեինի և դես-գամմա կարբոքսիպրոտրոմբինի մակարդակներ)[35], նրանց գնահատումը պահանջում է լյարդի վիզուալիզացիա ՀՇ կամ ՄՌՏ սկանավորման միջոցով: Այս սկանավորումները կատարվում են ներերակային կոնտրաստային նյութով, լյարդի արյունամատակարարման տարբեր փուլերում: ԼԲՔ-ի արյան հոսքի բնորոշ օրինաչափությունը թույլ են տալիս վերջնականապես հայտնաբերել լյարդաբջջային քաղցկեղը: Որպես այլընտրանք, սկանավորումը կարող է հայտնաբերել անորոշ ախտահարումներ, որոնք հետագա գնահատման համար կարելի է իրականացվել լյարդի բիոպսիա:[16][36]
Պատկերավորում[խմբագրել | խմբագրել կոդը]

Ուլտրաձայնային հետազոտությունը, ՀՇ և ՄՌՏ կարող են օգտագործվել լյարդաբջջային քաղցկեղը գնահատելու համար: ՀՇ և ՄՌՏ հետազոտությունների դեպքում ԼԲՔ-ը կարող է ունենալ աճի երեք հստակ օրինաչափություն՝
- Միայնակ մեծ ուռուցք
- Բազմակի ուռուցքներ
- Ոչ հստակ, ինֆիլտրատիվ աճի պատկերով ուռուցք
Համակարգային ՀՇ ախտորոշման զգայունությունը 68% (95% CI 55–80%) է, իսկ սպեցիֆիկությունը՝ 93% (95% CI 89–96%)՝ համեմատելով պաթոլագիական հետազոտությունների հետ։ Եռափուլ ՀՇ-ի դեպքում զգայունությունը եղել է 90% կամ ավելի բարձր, սակայն այս տվյալները չեն հաստատվել դիահերձման ուսումնասիրություններով[34]։
Այնուամենայնիվ, ՄՌՏ-ն ունի առանց իոնացնող ճառագայթման լյարդի բարձր որակի պատկերներ տրամադրելու առավելություն: ԼԲՔ-ն նկարագրվում է որպես բարձր ինտենսիվության T2 պատկեր, իսկ T1-ում ցածր ինտենսիվության պատկեր: ՄՌՏ-ի առավելությունն այն է, որ այն ունի բարելավված զգայունություն և յուրահատկություն համեմատած ուլտրաձային և ՀՇ-ի հետ, որոնց դեպքում դժվար է տարբերակել ԼԲՔ-ը ռեգեներացիոն հանգույցներից: Համակարգված վերանայումը ցույց տվեց, որ զգայունությունը 81% էր (95% CI 70–91%), իսկ սպեցիֆիկությունը՝ 85% (95% CI 77–93%)՝ համեմատած արտամղված կամ ռեզեկցիոն լյարդի պաթոլոգիական հետազոտության հետ՝ որպես հղման ստանդարտ[34]։ Զգայունությունն ավելի է մեծանում գադոլինիումի կոնտրաստի կիրառման և դիֆուզիոն պատկերներ:
Մագնիսառեզոնանսային տոմոգրաֆիան ավելի զգայուն և սպեցիֆիկ է քան համակարգչային ծերտագրությունը.[37]։
Ռադիոլոգները կասկածելի վնասվածքների համար օգտագործում են ստանդարտացված համակարգեր: Կատեգորիաները տատանվում են LI-RADS (LR) 1-ից մինչև 5, ըստ քաղցկեղի հավանականության[38] Եթե առկա են պատկերավորման որոշակի բավարար չափանիշներ, ապա ԼԲՔ ախտորոման հաստատման համար բիոպսիա չի պահանջվում[16]։
Ախտաֆիզիոլոգիա[խմբագրել | խմբագրել կոդը]

Լյարդի քաղցկեղը մակրոսկոպիկ բնութագրվում է որպես հանգույցավոր կամ ինֆիլտրատիվ ուռուցք: Հանգույցային տիպը կարող է լինել միայնակ (մեծ գոյացություն) կամ բազմակի (երբ զարգանում է որպես ցիռոզի բարդություն)։ Ուռուցքային հանգույցները կլոր կամ օվալ, մոխրագույն կամ կանաչ են (եթե ուռուցքն արտադրում է լեղի), լավ շրջագծված են, բայց պատիճավորված չեն: Դիֆուզ տեսակը վատ եզրագծված է և ներթափանցում է դռներակ կամ լյարդային երակներ (հազվադեպ)[16]։
Միկրոսկոպիկ լյարդաբջջային քաղցկեղի չորս կառուցվածքային և բջջաբանական տեսակներն են առանձնացվում՝ ֆիբրոլամելյար, պսևդոգլանդուլյար (ադենոիդ), պլեոմորֆ (հսկա բջիջային) և մաքուր բջիջային: Լավ տարբերակված ուռուցքային բջիջները նման են հեպատոցիտներին, ձևավորում են տրաբեկուլներ, լարեր և ցանցեր և ցիտոպլազմայում կարող են պարունակել լեղու պիգմենտ: Վատ տարբերակված ձևերում չարորակ էպիթելի բջիջները լինում են դիսկոհեզիվ, պլեոմորֆ, անապլաստիկ և հսկա։ Ուռուցքն ունի սակավ ստրոմա և վատ անոթավորման պատճառով կենտրոնական նեկրոզ[39]։ Հինգերորդ նկարագրված ձևը լիմֆոէպիթելիոման է (հեպատոցելուլյար քաղցկեղ)[40][41]։
-
 Լավ տարբերակված ԼԲՔ
Լավ տարբերակված ԼԲՔ -
 Չափավոր տարբերակված ԼԲՔ
Չափավոր տարբերակված ԼԲՔ -
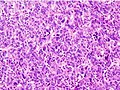 Վատ տարբերակված ԼԲՔ
Վատ տարբերակված ԼԲՔ



Փուլավորում[խմբագրել | խմբագրել կոդը]
Լյարդաբջջային քաղցկեղի կանխատեսման վրա ազդում է ուռուցքի փուլը և լյարդի ֆունկցիան՝ կապված լյարդի ցիռոզի հետ[42]։
Հասանելի են ԼԲՔ-ի փուլի մի շարք դասակարգումներ: ԼԲՔ-ի դասակարգման համակարգը պետք է ներառի ուռուցքի չափը և քանակը, անոթային ինվազիայի և արտալյարդային տարածման առկայությունը, լյարդի ֆունկցիան (շիճուկային բիլիռուբինի, ալբումին մակարդակը , ասցիտի առկայություն և պորտալ հիպերտենզիան) և հիվանդի ընդհանուր առողջական վիճակը[42]։
Փուլի դասակարգման առկա բոլոր համակարգերից Բարսելոնայի կլինիկայի լյարդի քաղցկեղի փուլավորման դասակարգումը ներառում է վերը նշված բոլոր բնութագրերը: Այս փուլային դասակարգումը կարող է օգտագործվել բուժման համար[43]։
| փուլ | նկարագրություն | Չայլդ-Պրուի դաս | ԱԿՈՒԽ դկարգավիճակ |
|---|---|---|---|
| 0 (շատ վաղ փուկ) | եզակի հանգույց, < 3սմ | A | 0 |
| A (վաղ փուլ) | 1–3 հանգույց, բոլորը < 3սմ | A կամ B | |
| B (միջանկյալ փուլ) | բազմահանգույցային | ||
| C (ուշ փուլ) | դռներակի ինվազիա և արտալյարդային տարածում | 1 կամ 2 | |
| D (տերմինալ փուլ) | լյարդի սուր վնասում | C | 3 կամ 4 |
Ուռուցքի կԿարևոր առանձնահատկություններն են՝
- չափ
- տարածում
- լյարդային անոթների ինվազիա
- ուռուցքի պատիճի առկայություն
- արտալյարդային մետաստազների առկայություն
- սուդտր հանգույցների առկայություն
- ուռուցքի անոթավորում
Ուռուցքի պատիճը գնահատելու համար ՄՌՏ-ն համարվում է լավագոյն մեթոդը
Մետաստազների ամենատարածված վայրերն են թոքերը, որովայնի ավշային հանգույցները և ոսկրերը[47]։
կանխարգելում[խմբագրել | խմբագրել կոդը]
Քանի որ հեպատիտ B-ն և C-ն լյարդաբջջային քաղցկեղի հիմնական պատճառներն են, վարակի կանխարգելումը առանցքային է ԼԲՔ-ի կանխարգելման համար: Այսպիսով, հեպատիտ B-ի դեմ մանկական տարիքում պատվաստումը կարող է ապագայում նվազեցնել լյարդի քաղցկեղի վտանգը[48]։ Ցիռոզով հիվանդները պետք է խուսափեն ալկոհոլի օգտագործումից։ Բացի այդ, որոշ հիվանդների համար կարող է օգտակար լինել հեմոքրոմատոզի սկրինինգը[49]։
- Բուժական նպատակ. սահմանափակված հիվանդության դեպքում, երբ քաղցկեղը սահմանափակվում է լյարդի մեկ կամ մի քանի հատվածով, չարորակ բջիջների վիրահատական հեռացումը կարող է բուժիչ լինել: Սա կարող է իրականացվել լյարդի ախտահարված հատվածի ռեզեկցիայով (մասնակի հեպատէկտոմիա) կամ որոշ դեպքերում ամբողջ օրգանի օրթոտոպիկ փոխպատվաստմամբ:
- "Bridging" intention: for limited disease which qualifies for potential liver transplantation, the person may undergo targeted treatment of some or all of the known tumor while waiting for a donor organ to become available.[50]
- "Downstaging" intention: for moderately advanced disease which has not spread beyond the liver, but is too advanced to qualify for curative treatment. The person may be treated by targeted therapies in order to reduce the size or number of active tumors, with the goal of once again qualifying for liver transplant after this treatment.[50]
- Palliative intention: for more advanced disease, including spread of cancer beyond the liver or in persons who may not tolerate surgery, treatment intended to decrease symptoms of disease and maximize duration of survival.
Loco-regional therapy (also referred to as liver-directed therapy) refers to any one of several minimally-invasive treatment techniques to focally target HCC within the liver. These procedures are alternatives to surgery, and may be considered in combination with other strategies, such as a later liver transplantation.[51] Generally, these treatment procedures are performed by interventional radiologists or surgeons, in coordination with a medical oncologist. Loco-regional therapy may refer to either percutaneous therapies (e.g. cryoablation), or arterial catheter-based therapies (chemoembolization or radioembolization).[փա՞ստ]
Բուժում[խմբագրել | խմբագրել կոդը]
Հեպատոցելուլյար քաղցկեղի բուժումը կախված է հիվանդության փուլից, վիրահատություն իրականացնելու հնարավորությունից և լյարդի փոխպատվաստման Հասանելիությունից։
Վիրաբուժական ռեզեկցիա[խմբագրել | խմբագրել կոդը]

Ուռուցքի վիրաբուժական հեռացումը կապված է քաղցկեղի ավելի լավ կանխատեսման հետ, սակայն հիվանդների միայն 5-15%-ն է կատարվում վիրահատական ռեզեկցիա՝ հիվանդության տարածման կամ լյարդի վատ ֆունկցիայի պատճառով[52]։ Վիրահատությունը դիտարկվում է միայն այն դեպքում, եթե ամբողջ ուռուցքը կարող է ապահով կերպով հեռացվել՝ պահպանելով լյարդի բավարար ֆունկցիոնալություն: Նախավիրահատական պատկերավորումը կարևոր է թե՛ ԼԲՔ-ի չափը որոշելու և թե՛ վիրահատությունից հետո մնացած լյարդի մնացորդային քանակությունը գնահատելու համար: Լյարդի ֆունկցիան պահպանելու համար լյարդի մնացորդային ծավալը ոչ ցիռոզ լյարդի դեպքում պետք է գերազանցի լյարդի ընդհանուր ծավալի 25%-ը, իսկ ցիռոտիկ լյարդի դեպքում՝ ավելի քան 40%[53]։ Վիրահատությունը դիտարկվում է միայն այն դեպքում, եթե ամբողջ ուռուցքը կարող է ապահով կերպով հեռացվել՝ պահպանելով լյարդի բավարար ֆունկցիոնալություն: Նախավիրահատական պատկերավորումը կարևոր է թե՛ ԼԲՔ-ի չափը որոշելու և թե՛ վիրահատությունից հետո մնացած լյարդի մնացորդային քանակությունը գնահատելու համար: Լյարդի ֆունկցիան պահպանելու համար լյարդի մնացորդային ծավալը ոչ ցիռոզ լյարդի դեպքում պետք է գերազանցի լյարդի ընդհանուր ծավալի 25%-ը, իսկ ցիռոտիկ լյարդի դեպքում՝ ավելի քան 40%: Հիվանդ կամ ցիռոտիկ լյարդի վիրահատությունը սովորաբար կապված է ավելի բարձր հիվանդացության և մահացության հետ: Ռեզեկցիայից հետո ռեցիդիվների հաճխությունը կազմում է 50-60%: Սինգապուրի լյարդի քաղցկեղի կրկնության սանդղակը կարող է օգտագործվել վիրահատությունից հետո կրկնվելու ռիսկը գնահատելու համար[54]։
Լյարդի փոխպատվաստում[խմբագրել | խմբագրել կոդը]
Լյարդի փոխպատվաստումը, փոխարինելով հիվանդ լյարդը դիակի կամ կենդանի դոնորի լյարդով, աճող դեր է խաղում ԼԲՔ-ի բուժման մեջ: Թեև լյարդի փոխպատվաստման արդյունքներն ի սկզբանե վատ էին (20%-36% ապրելիության մակարդակ)[16], , արդյունքները զգալիորեն բարելավվել են վիրաբուժական տեխնիկայի բարելավմամբ և ԱՄՆ փոխպատվաստման կենտրոններում Միլանի չափանիշների ընդունմամբ: Չինաստանում Շանհայի ընդլայնված չափանիշները հանգեցրել են ընդհանուր ապրելիությաան և հիվանդություն անկախ ապրելիության ցուցանիշների բարձրացմանը: 2000-ականների վերջին կատարված ուսումնասիրությունները ցույց են տվել ապրելիության ավելի բարձր մակարդակ՝ 67%-ից մինչև 91%[55]։
ԼԼյարդի փոխպատվաստման ռիսկերը գերազանցում են բուն ընթացակարգի ռիսկը: Դոնորական լյարդի մերժումը կանխելու համար կիրառվող իմունոսուպրեսիվ դեղամիջոցները խաթարում են դիսֆունկցիոնալ բջիջների դեմ օրգանիզմի բնական պայքարը: Եթե մինչև փոխպատվաստումը ուռուցքը լյարդից դուրս չբացահայտված տարածում ունի, ապա այս դեղամիջոցները արդյունավետորեն մեծացնում է հիվանդության առաջընթացի արագությունը և նվազեցնում ապրելիությունը: Սա նկատի ունենալով, լյարդի փոխպատվաստումը կարող է բուժիչ մոտեցում լինել ԼԲՔ ունեցող այն հիվանդների համար, ովքեր չունեն արտալյարդային մետաստազներ: Հիվանդի ընտրությունը համարվում է հաջողության գլխավոր բանալի.[56]։
Աբլացիա[խմբագրել | խմբագրել կոդը]
- Ռադիոհաճախային աբլյացիայի դեպքում օգտագործվում է բարձր հաճախականության ռադիոալիքներ, որոնք ունեն լոկալ ազդեցոություն ուռուցքի վրա: Էլեկտրոդներն ուլտրաձայնային հետազոտության հսկողությամբ տեղադրվում են լյարդի ուռուցքի մեջ՝ օգտագործելով միջմաշկային, լապարոսկոպիկ կամ բաց վիրաբուժական մոտեցում: Այն հարմար է փոքր ուռուցքների համար (<5 սմ): Ռադիոհաճախային աբլյացիայի լավագույն արդյունքները դիտվում են 4 սմ-ից փոքր միայնակ ուռուցք ունեցող հիվանդների մոտ[57]։ Քանի որ այն տեղային բուժման մեթոդ է և ունի նվազագույն ազդեցություն հարակից առողջ հյուսվածքների վրա, այն կարող է կրկնվել մի քանի անգամ: Ավելի փոքր ուռուցք ունեցողների համար ապրելիության ցուցանիշը ավելի բարձր է: 302 հիվանդների շրջանում կատարված ուսումնասիրություններում 5 սմ, 2,1-ից 5 սմ և ≤2 սմ ախտահարումներ ունեցողների եռամյա ապրելիության մակարդակը համապատասխանաբար եղել է 59, 74 և 91%:[58] Ավելի մեծ ռանդոմիզացված փորձարկումը, որը համեմատում էր փոքր ԼԲՔ-ի հհիվանդների շրջանում վիրաբուժական մասնահատումը և ռադիոհաճախային աբլացիան, ՌՀԱ-ով բուժվող հիվանդների համար ցույց տվեց նույնատիպ չորս տարվա ապրելիություն և ավելի քիչ հիվանդացություն[59]։
- Կրիոաբլյացիան մեթոդ է, որի դեպքում ուռուցքային հյուսվածքը ոչնչացնելու համար օգտագործվում է ցածր ջերմաստիճան։ Ուռուցքը չի հեռացվում, իսկ ոչնչացված քաղցկեղը ներծծվում է օրգանիզմի կողմից: Լյարդի անվիրահատելի ուռուցքներով հիվանդների մոտ նախնական արդյունքները համարժեք են ռեզեկցիայի արդյունքներին: Կրիովիրաբուժության դեպքում չժանգոտվող պողպատից զոնդը տեղադրվում է ուռուցքի կենտրոնական հատվածում: Հեղուկ ազոտը շրջանառվում է այս սարքի ծայրով: Ուռուցքը և կես դյույմ եզրագիծով նորմալ լյարդային հյուսվածքը 15 րոպե տևողությամբ սառեցվում է մինչև -190 °C , ինչը մահացու է բոլոր հյուսվածքների համար: Տվյալ հատվածը հալեցվում է 10 րոպե, այնուհետև ևս 15 րոպե սառեցվում մինչև −190 °C : Ուռուցքի հալվելուց հետո զոնդը հանվում է, վերահսկվում է արյունահոսությունը և պրոցեդուրան ավարտվում է: Հիվանդը հետվիրահատական առաջին գիշերն անցկացնում է վերակենդանացման բաժանմունքում և սովորաբար 3-5 օր անց դուրս է գրվում: Հաճախ կրիովիրաբուժությունն օգտագործվում է լյարդի ռեզեկցիայի հետ համատեղ։
- Մաջմաշկային էթանոլային ներարկումը լավ տանելի է փոքր (<3 սմ) միայնակ ուռուցքների դեպքում; 2005թ.-ի դրությամբ ոչ մի ռանդոմիզացված փորձարկում չի համեմատել ռեզեկցիան միջմաշկային բուժման հետ։ ռեցիդիվների հաճախականությունը նման է հետվիրահատականին: Այնուամենայնիվ, համեմատական ուսումնասիրությունները ցույց են տվել, որ փոքր ԼԲՔ ունեցող հիվանդների համար տեղային թերապիայի դեպքում 5-ամյա ապրելիության մակարդակը կարող է հասնել մոտ 60%[60]։
Arterial catheter-based treatment[խմբագրել | խմբագրել կոդը]
- Transcatheter arterial chemoembolization (TACE) is performed for unresectable tumors or as a temporary treatment while waiting for liver transplant ("bridge to transplant"). TACE is done by injecting an antineoplastic drug (e.g. cisplatin) mixed with a radio-opaque contrast (e.g. Lipiodol) and an embolic agent (e.g. Gelfoam) into the right or left hepatic artery via the groin artery. The goal of the procedure is to restrict the tumor's vascular supply while supplying a targeted chemotherapeutic agent. TACE has been shown to increase survival and to downstage HCC in patients who exceed the Milan criteria for liver transplant. Patients who undergo the procedure are followed with CT scans and may need additional TACE procedures if the tumor persists.[61] As of 2005, multiple trials show objective tumor responses and slowed tumor progression, but questionable survival benefit compared to supportive care; greatest benefit is seen in people with preserved liver function, absence of vascular invasion, and smallest tumors. TACE is not suitable for big tumors (>8 cm), the presence of portal vein thrombus, tumors with a portal-systemic shunt, and patients with poor liver function.[փա՞ստ]
- Selective internal radiation therapy (SIRT) can be used to destroy the tumor from within (thus minimizing exposure to healthy tissue). Similar to TACE, this is a procedure in which an interventional radiologist selectively injects the artery or arteries supplying the tumor with a chemotherapeutic agent. The agent is typically Yttrium-90 (Y-90) incorporated into embolic microspheres that lodge in the tumor vasculature, causing ischemia and delivering their radiation dose directly to the lesion. This technique allows for a higher, local dose of radiation to be delivered directly to the tumor while sparing normal healthy tissue. While not curative, patients have increased survival. No studies have been done to compare whether SIRT is superior to TACE in terms of survival outcomes, although retrospective studies suggest similar efficacy.[62] Two products are available, SIR-Spheres and TheraSphere. The latter is an FDA-approved treatment for primary liver cancer (HCC) which has been shown in clinical trials to increase the survival rate of low-risk patients. SIR-Spheres are FDA-approved for the treatment of metastatic colorectal cancer, but outside the US, SIR-Spheres are approved for the treatment of any nonresectable liver cancer including primary liver cancer.[63]
External beam therapy[խմբագրել | խմբագրել կոդը]
- The role of radiotherapy in the treatment of hepatocellular carcinoma has evolved as technological advancements in treatment delivery and imaging have provided a means for safe and effective radiotherapy delivery in a wide spectrum of HCC patients. In metastatic cases, radiotherapy can be used for palliative care.[64][65]
- Proton therapy for unresectable hepatocellular carcinoma was associated with improved survival relative to photon-based radiation therapy which may be driven by decreased incidence of post-treatment liver decompensation[66] and a number of randomized controlled trials are currently ongoing.[67][68][69]
Systemic[խմբագրել | խմբագրել կոդը]
In disease which has spread beyond the liver, systemic therapy may be a consideration. In 2007, Sorafenib, an oral multikinase inhibitor, was the first systemic agent approved for first-line treatment of advanced HCC.[70] Trials have found modest improvement in overall survival: 10.7 months vs 7.9 months and 6.5 months vs 4.2 months.[71][70]
The most common side effects of Sorafenib include a hand-foot skin reaction and diarrhea.[71] Sorafenib is thought to work by blocking growth of both tumor cells and new blood vessels. Numerous other molecular targeted drugs are being tested as alternative first- and second-line treatments for advanced HCC.[72]
A host of additional targeted therapies and immune checkpoint inhibitors have been found to be effective against this disease. For instance, in the recent phase III trial IMBrave 150, the combination of atezolizumab and bevacizumab was found to improve both overall and progression-free survival compared to sorafenib alone.[73]
Tremelimumab (Imjudo) was approved for medical use in the United States in October 2022.[74] It is indicated, in combination with durvalumab, for the treatment of adults with unresectable hepatocellular carcinoma.[74]
Other[խմբագրել | խմբագրել կոդը]
- Portal vein embolization (PVE): This technique is sometimes used to increase the volume of healthy liver, in order to improve chances of survival following surgical removal of diseased liver. For example, embolization of the right main portal vein would result in compensatory hypertrophy of the left lobe, which may qualify the patient for a partial hepatectomy. Embolization is performed by an interventional radiologist using a percutaneous transhepatic approach. This procedure can also serve as a bridge to transplant.[75]
- High intensity focused ultrasound (HIFU) (as opposed to diagnostic ultrasound) is an experimental technique which uses high-powered ultrasound waves to destroy tumor tissue.
- A systematic review assessed 12 articles involving a total of 318 patients with hepatocellular carcinoma treated with Yttrium-90 radioembolization.[76] Excluding a study of only one patient, post-treatment CT evaluation of the tumor showed a response ranging from 29 to 100% of patients evaluated, with all but two studies showing a response of 71% or greater.
Կանխատեսում[խմբագրել | խմբագրել կոդը]
Սովորական կանխատեսումը վատ է, քանի որ լյարդաբջջային կարցինոմայի միայն 10-20%-ը կարող է ամբողջությամբ հեռացվել վիրահատության միջոցով: Եթե քաղցկեղը հնարավոր չէ ամբողջությամբ հեռացնել, հիվանդությունը սովորաբար մահացու ելք է ունենում 3-6 ամսվա ընթացքում[77]։ Սա մասամբ պայմանավորված է ուռուցքով հիվանդների ուշ դիմելիությամբ, ինչպես նաև ԼԲՔ-ի բարձր տարածվածություն ունեցող մարզերում բժշկական փորձի և հաստատությունների բացակայությամբ: Այնուամենայնիվ, ապրելիությունը կարող է տարբեր լինել, և երբեմն կարող է հասնել 6 ամիս կամ ավելի:
Համաճարակաբանություն[խմբագրել | խմբագրել կոդը]


ԼԲՔ-ը աշխարհում ամենատարածված ուռուցքներից մեկն է: Տղամարդիկ ավելի շատ են հիվանդանում, քան կանայք։Հիվանդությունը առավելապես դիտվում է 30-ից 50 տարեկանների շրջանում:[80] Հեպատոցելուլյար քաղցկեղը ամբողջ աշխարհում տարեկան 662,000 մահվան պատճառ է դառնում[81], որի մոտ կեսը գրանցվում է Չինաստանում։
Africa and Asia[խմբագրել | խմբագրել կոդը]
In some parts of the world, such as sub-Saharan Africa and Southeast Asia, HCC is the most common cancer, generally affecting men more than women, and with an age of onset between the late teens and 30s.[16] This variability is in part due to the different patterns of hepatitis B and hepatitis C transmission in different populations – infection at or around birth predispose to earlier cancers than if people are infected later. The time between hepatitis B infection and development into HCC can be years, even decades, but from diagnosis of HCC to death, the average survival period is only 5.9 months according to one Chinese study during the 1970-80s, or 3 months (median survival time) in sub-Saharan Africa according to Manson's textbook of tropical diseases. HCC is one of the deadliest cancers in China, where chronic hepatitis B is found in 90% of cases. In Japan, chronic hepatitis C is associated with 90% of HCC cases. Foods infected with Aspergillus flavus (especially peanuts and corns stored during prolonged wet seasons) which produces aflatoxins pose another risk factor for HCC.[փա՞ստ]
North America and Western Europe[խմբագրել | խմբագրել կոդը]
The most common malignant tumors in the liver represent metastases (spread) from tumors which originate elsewhere in the body.[80] Among cancers that originate from liver tissue, HCC is the most common primary liver cancer. In the United States, the US surveillance, epidemiology, and end results database program, shows that HCC accounts for 65% of all cases of liver cancers.[82] As screening programs are in place for high-risk persons with chronic liver disease, HCC is often discovered much earlier in Western countries than in developing regions such as sub-Saharan Africa.[փա՞ստ]
Acute and chronic hepatic porphyrias (acute intermittent porphyria, porphyria cutanea tarda, hereditary coproporphyria, variegate porphyria) and tyrosinemia type I are risk factors for hepatocellular carcinoma. The diagnosis of an acute hepatic porphyria (AIP, HCP, VP) should be sought in patients with HCC without typical risk factors of hepatitis B or C, alcoholic liver cirrhosis, or hemochromatosis. Both active and latent genetic carriers of acute hepatic porphyrias are at risk for this cancer, although latent genetic carriers have developed the cancer at a later age than those with classic symptoms. Patients with acute hepatic porphyrias should be monitored for HCC.[փա՞ստ]
The incidence of HCC is relatively lower in the Western Hemisphere than in Eastern Asia. However, despite the statistics being low, the diagnosis of HCC has increased since the 1980s and it is continuing to increase, making it one of the rising causes of death due to cancer. The common risk factor for HCC is hepatitis C, along with other health issues.[83][84]
Research[խմբագրել | խմբագրել կոդը]
Preclinical[խմբագրել | խմբագրել կոդը]
Mipsagargin (G-202), has orphan drug designation as a treatment during chemotherapy for HCC.[85] It is a thapsigargin-based prodrug with cytotoxic activity used to reduce blood flow to the tumor during treatment. Results from Phase 2 trial recommended G-202 as a first-in-class PSMA-targeted prodrug and that it move to clinical trials.[86]
Current research includes the search for the genes that are disregulated in HCC, antiheparanase antibodies,[87] protein markers,[88] non-coding RNAs[89] (such as TUC338)[90] and other predictive biomarkers.[91][92] As similar research is yielding results in various other malignant diseases, it is hoped that identifying the aberrant genes and the resultant proteins could lead to the identification of pharmacological interventions for HCC.[93]
The development of three-dimensional culture methods provides a new approach for preclinical studies of cancer therapy using patient-derived organoids. These miniaturized organoid 'avatars' of a patient's tumor recapitulate several features of the original tumor, rendering them an attractive model for drug-sensitivity testing and precision medicine for HCC and other types of primary liver cancer.[94]
Furthermore, HCC occurs in patients with liver disease. A biomarker named six-miRNA signature allows effective treatment of patients with HCC and is able to predict its recurrence in the liver.[95]
Clinical[խմբագրել | խմբագրել կոդը]
JX-594, an oncolytic virus, has orphan drug designation for this condition and is undergoing clinical trials.[96] Hepcortespenlisimut-L (Hepko-V5), an oral cancer vaccine, also has US FDA orphan drug designation for HCC.[97] Immunitor Inc. completed a Phase II trial, published in 2017.[98] A randomized trial of people with advanced HCC showed no benefit for the combination of everolimus and pasireotide.[99]
References[խմբագրել | խմբագրել կոդը]
- ↑ Forner A, Llovet JM, Bruix J (2012). «Hepatocellular carcinoma». The Lancet. 379 (9822): 1245–1255. doi:10.1016/S0140-6736(11)61347-0. PMID 22353262. S2CID 24927898.
- ↑ «Global Cancer Observatory». gco.iarc.fr. Վերցված է 2021-06-24-ին.
- ↑ 3,0 3,1 Kumar V, Fausto N, Abbas A, eds. (2015). Robbins & Cotran Pathologic Basis of Disease (9th ed.). Saunders. էջեր 870–873. ISBN 978-1455726134.
- ↑ «Liver cancer overview». Mayo Clinic.
- ↑ 5,0 5,1 Heidelbaugh, Joel J.; Bruderly, Michael (2006-09-01). «Cirrhosis and chronic liver failure: part I. Diagnosis and evaluation». American Family Physician. 74 (5): 756–762. ISSN 0002-838X. PMID 16970019.
- ↑ Alter MJ (2007). «Epidemiology of hepatitis C virus infection». World Journal of Gastroenterology. 13 (17): 2436–41. doi:10.3748/wjg.v13.i17.2436. PMC 4146761. PMID 17552026.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ White DL, Kanwal F, El-Serag HB (2012). «Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review». Clinical Gastroenterology and Hepatology. 10 (12): 1342–59. doi:10.1016/j.cgh.2012.10.001. PMC 3501546. PMID 23041539.
- ↑ «NAFLD vs. NASH». Medicine Specifics (ամերիկյան անգլերեն). 2019-11-11. Վերցված է 2021-06-22-ին.
- ↑ 9,0 9,1 9,2 El–Serag HB; Hampel H; Javadi F (2006). «the association between diabetes and hepatocellular carcinoma: a systematic review of epidemiological evidence». Clinical Gastroenterology and Hepatology. 4 (3): 369–380. doi:10.1016/j.cgh.2005.12.007. PMID 16527702. «Diabetes is associated with an increased risk for HCC. However, more research is required to examine issues related to the duration and treatment of diabetes, and confounding by diet and obesity»
- ↑ Wang XW, Hussain SP, Huo TI, Wu CG, Forgues M, Hofseth LJ, Brechot C, Harris CC (2002). «Molecular pathogenesis of human hepatocellular carcinoma». Toxicology. 181–182: 43–47. doi:10.1016/S0300-483X(02)00253-6. PMID 12505283. «Recent studies in our laboratory have identified several potential factors that may contribute to the pathogenesis of HCC...For example, oxyradical overload diseases such as Wilson disease and hemochromatosis result in the generation of oxygen/nitrogen species that can cause mutations in the p53 tumour suppressor gene»
- ↑ Cheng W, Govindarajan S, Redeker A (1992). «Hepatocellular carcinoma in a case of Wilson's disease». Liver International. 12 (1): 42–45. doi:10.1111/j.1600-0676.1992.tb00553.x. PMID 1314321. «The patient described here was the oldest and only the third female patient with hepatocellular carcinoma complicating Wilson's disease to be reported in the literature»
- ↑ Wilkinson ML, Portmann B, Williams R (1983). «Wilson's disease and hepatocellular carcinoma: possible protective role of copper». Gut. 24 (8): 767–771. doi:10.1136/gut.24.8.767. PMC 1420230. PMID 6307837. «As copper has been shown to protect against chemically induced hepatocellular carcinoma in rats, this may be the reason for the extreme rarity of hepatocellular carcinoma in patients with Wilson's disease and possibly in other liver diseases with hepatic copper overload»
- ↑ Huang YC, Tsan YT, Chan WC, Wang JD, Chu WM, Fu YC, Tong KM, Lin CH, Chang ST, Hwang WL (2015). «Incidence and survival of cancers among 1,054 hemophilia patients: A nationwide and 14-year cohort study». American Journal of Hematology. 90 (4): E55–E59. doi:10.1002/ajh.23947. PMID 25639564.
- ↑ Shetty, Shrimati; Sharma, Nitika; Ghosh, Kanjaksha (2016-03-01). «Epidemiology of hepatocellular carcinoma (HCC) in hemophilia». Critical Reviews in Oncology/Hematology (անգլերեն). 99: 129–133. doi:10.1016/j.critrevonc.2015.12.009. ISSN 1040-8428. PMID 26754251.
- ↑ Tanaka M, Katayama F, Kato H, Tanaka H, Wang J, Qiao YL, Inoue M (2011). «Hepatitis B and C virus infection and hepatocellular carcinoma in China: A review of epidemiology and control measures». Journal of Epidemiology. 21 (6): 401–416. doi:10.2188/jea.JE20100190. PMC 3899457. PMID 22041528.
- ↑ 16,00 16,01 16,02 16,03 16,04 16,05 16,06 16,07 16,08 16,09 Balogh J, Victor D, Asham E, Burroughs S, Boktour M, Saharia A, Li X, Ghobrial M, Monsour H (2016). «Hepatocellular carcinoma: a review». Journal of Hepatocellular Carcinoma. 3: 41–53. doi:10.2147/JHC.S61146. PMC 5063561. PMID 27785449.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ «Pathophysiology». 2019-11-10. Վերցված է May 12, 2010-ին.
{{cite journal}}: Cite journal requires|journal=(օգնություն) - ↑ 18,0 18,1 18,2 Hassan MM, Curley SA, Li D, Kaseb A, Davila M, Abdalla EK, Javle M, Moghazy DM, Lozano RD, Abbruzzese JL, Vauthey JN (2010). «Association of diabetes duration and diabetes treatment with the risk of hepatocellular carcinoma». Cancer. 116 (8): 1938–1946. doi:10.1002/cncr.24982. PMC 4123320. PMID 20166205. «Diabetes appears to increase the risk of HCC, and such risk is correlated with a long duration of diabetes. Relying on dietary control and treatment with sulfonylureas or insulin were found to confer the highest magnitude of HCC risk, whereas treatment with biguanides or thiazolidinediones was associated with a 70% HCC risk reduction among diabetics.»
- ↑ 19,0 19,1 Donadon, Valter (2009). «Antidiabetic therapy and increased risk of hepatocellular carcinoma in chronic liver disease». World Journal of Gastroenterology. 15 (20): 2506–11. doi:10.3748/wjg.15.2506. PMC 2686909. PMID 19469001. «Our study confirms that type 2 diabetes mellitus is an independent risk factor for HCC and pre-exists in the majority of HCC patients. Moreover, in male patients with type 2 diabetes mellitus, our data shows a direct association of HCC with insulin and sulphanylureas treatment and an inverse relationship with metformin therapy.»
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Donadon V, Balbi M, Ghersetti M, և այլք: (2009). «Antidiabetic therapy and increased risk of hepatocellular carcinoma in chronic liver disease». World Journal of Gastroenterology. 15 (20): 2506–11. doi:10.3748/wjg.15.2506. PMC 2686909. PMID 19469001.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Siegel A, Zhu AX (2009). «Metabolic Syndrome and hepatocellular carcinoma». Cancer. 115 (24): 5651–5661. doi:10.1002/cncr.24687. PMC 3397779. PMID 19834957. «The majority of 'cryptogenic' HCC in the United States is attributed to nonalcoholic fatty liver disease (NAFLD), a hepatic manifestation of the metabolic syndrome... It is predicted that metabolic syndrome will lead to large increases in the incidence of HCC over the next decades. A better understanding of the relation between these two diseases ultimately should lead to improved screening and treatment options for patients with HCC.»
- ↑ Stickely F, Hellerbrand C (2010). «Non-alcoholic fatty liver disease as a risk factor for hepatocellular carcinoma: mechanisms and implications». Gut. 59 (10): 1303–1307. doi:10.1136/gut.2009.199661. PMID 20650925. S2CID 31016985. «Based on the known association of NAFLD with IR and MS, approximately two-thirds of the patients were obese and/or diabetic, 4 and a remarkable 25% of these patients had no cirrhosis... Therefore, it is particularly worrying that the most persuasive evidence for an association between NAFLD and HCC derives from studies on the risk of HCC in patients with metabolic syndrome»
- ↑ «Hepatocellular Carcinoma and Diseases». Վերցված է May 12, 2010-ին.
- ↑ Höpfner M, Huether A, Sutter AP, Baradari V, Schuppan D, Scherübl H (2006). «Blockade of IGF-1 receptor tyrosine kinase has antineoplastic effects in hepatocellular carcinoma cells». Biochemical Pharmacology. 71 (10): 1435–1448. doi:10.1016/j.bcp.2006.02.006. PMID 16530734. «Inhibition of IGF-1R tyrosine kinase (IGF-1R-TK) by NVP-AEW541 induces growth inhibition, apoptosis and cell cycle arrest in human HCC cell lines without accompanying cytotoxicity. Thus, IGF-1R-TK inhibition may be a promising novel treatment approach in HCC.»
- ↑ Huynh H, Chow PK, Ooi LL, Soo KC (2002). «A possible role for insulin-like growth factor-binding protein-3 autocrine/paracrine loops in controlling hepatocellular carcinoma cell proliferation». Cell Growth & Differentiation. 13 (3): 115–122. PMID 11959812. «Our data indicate that loss of autocrine/paracrine IGFBP-3 loops may lead to HCC tumor growth and suggest that modulating production of the IGFs, IGFBP-3, and IGF-IR may represent a novel approach in the treatment of HCC.»
- ↑ Martin NM, Abu Dayyeh BK, Chung RT (2008). «Anabolic steroid abuse causing recurrent hepatic adenomas and hemorrhage». World Journal of Gastroenterology. 14 (28): 4573–4575. doi:10.3748/wjg.14.4573. PMC 2731289. PMID 18680242. «This is the first reported case of hepatic adenoma re-growth with recidivistic steroid abuse, complicated by life-threatening hemorrhage.»
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Gorayski P, Thompson CH, Subhash HS, Thomas AC (2007). «Hepatocellular carcinoma associated with recreational anabolic steroid use». British Journal of Sports Medicine. 42 (1): 74–75. doi:10.1136/bjsm.2007.03932. PMID 18178686. S2CID 21900098. «Malignant transformation to HCC from a pre-existing hepatic adenoma confirmed by immunohistochemical study has previously not been reported in athletes taking anabolic steroids. Further studies using screening programmes to identify high-risk individuals are recommended.»
- ↑ Shibata T, Aburatani H (2014). «Exploration of liver cancer genomes». Nat Rev Gastroenterol Hepatol. 11 (6): 340–9. doi:10.1038/nrgastro.2014.6. PMID 24473361. S2CID 8611393.
- ↑ Chien-Jen Chen; Hwai-I. Yang; Jun Su; Chin-Lan Jen; San-Lin You; Sheng-Nan Lu; Guan-Tarn Huang; Uchenna H. Iloeje (2006). «Risk of Hepatocellular Carcinoma Across a Biological Gradient of Serum Hepatitis B Virus DNA Level». JAMA. 295 (1): 65–73. doi:10.1001/jama.295.1.65. PMID 16391218.
- ↑ Yang SF, Chang CW, Wei RJ, Shiue YL, Wang SN, Yeh YT (2014). «Involvement of DNA damage response pathways in hepatocellular carcinoma». Biomed Res Int. 2014: 1–18. doi:10.1155/2014/153867. PMC 4022277. PMID 24877058.
- ↑ Nishida N, Kudo M (2013). «Oxidative stress and epigenetic instability in human hepatocarcinogenesis». Dig Dis. 31 (5–6): 447–53. doi:10.1159/000355243. PMID 24281019.
- ↑ Heimbach, Julie K.; Kulik, Laura M.; Finn, Richard; Sirlin, Claude B.; Abecassis, Michael; Roberts, Lewis R.; Zhu, Andrew; Murad, M. Hassan; Marrero, Jorge (2017-01-01). «Aasld guidelines for the treatment of hepatocellular carcinoma». Hepatology (անգլերեն). 67 (1): 358–380. doi:10.1002/hep.29086. ISSN 1527-3350. PMID 28130846.
- ↑ «Clinical features and diagnosis of primary hepatocellular carcinoma». UptoDate. Վերցված է 4 February 2014-ին.
- ↑ 34,0 34,1 34,2 Colli, A; Fraquelli, M; Casazza, G; Massironi, S; Colucci, A; Conte, D; Duca, P (March 2006). «Accuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic review». The American Journal of Gastroenterology. 101 (3): 513–23. doi:10.1111/j.1572-0241.2006.00467.x. PMID 16542288. S2CID 9563077.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Ertle, JM; Heider, D; Wichert, M; Keller, B; Kueper, R; Hilgard, P; Gerken, G; Schlaak, JF (2013). «A combination of α-fetoprotein and des-γ-carboxy prothrombin is superior in detection of hepatocellular carcinoma». Digestion. 87 (2): 121–31. doi:10.1159/000346080. PMID 23406785. S2CID 25266129.
- ↑ «Benign Liver Tumors». The Lecturio Medical Concept Library. Վերցված է 4 July 2021-ին.
- ↑ El-Serag HB, Marrero JA, Rudolph L, Reddy KR (May 2008). «Diagnosis and treatment of hepatocellular carcinoma». Gastroenterology. 134 (6): 1752–63. doi:10.1053/j.gastro.2008.02.090. PMID 18471552. S2CID 10418520.
- ↑ «Li-Rads». Արխիվացված է օրիգինալից 2017-07-11-ին. Վերցված է 2014-02-04-ին.
- ↑ Hepatocellular carcinoma (Photo) Արխիվացված 2021-11-01 Wayback Machine ATLAS OF PATHOLOGY
- ↑ Chan AW, Zhang Z, Chong CC, Tin EK, Chow C, Wong N (2019). «Genomic landscape of lymphoepithelioma-like hepatocellular carcinoma». J Pathol. 249 (2): 166–172. doi:10.1002/path.5313. PMID 31168847. S2CID 174815950.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Chan AW, Tong JH, Pan Y, Chan SL, Wong GL, Wong VW, Lai PB, To KF (2015). «Lymphoepithelioma-like hepatocellular carcinoma: an uncommon variant of hepatocellular carcinoma with favorable outcome». Am J Surg Pathol. 39 (3): 304–312. doi:10.1097/pas.0000000000000376. PMID 25675010. S2CID 40384842.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ 42,0 42,1 Duseja, Ajay (2014-08-01). «Staging of Hepatocellular Carcinoma». Journal of Clinical and Experimental Hepatology. 4 (Suppl 3): S74–S79. doi:10.1016/j.jceh.2014.03.045. PMC 4284240. PMID 25755615.
- ↑ Llovet JM, Brú C, Bruix J (1999). «Prognosis of hepatocellular carcinoma: the BCLC staging classification». Seminars in Liver Disease. 19 (3): 329–38. doi:10.1055/s-2007-1007122. PMID 10518312.
- ↑ «BCLC staging system and the Child-Pugh system ;Liver cancer ; Cancer Research UK». www.cancerresearchuk.org.
- ↑ «What is the Barcelona Clinic Liver Cancer (BCLC) system for hepatocellular carcinoma (HCC) staging?». www.medscape.com.
- ↑ Kinoshita, A; Onoda, H; Fushiya, N; Koike, K; Nishino, H; Tajiri, H (27 March 2015). «Staging systems for hepatocellular carcinoma: Current status and future perspectives». World Journal of Hepatology. 7 (3): 406–24. doi:10.4254/wjh.v7.i3.406. PMC 4381166. PMID 25848467.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Katyal, Sanjeev; Oliver, James H.; Peterson, Mark S.; Ferris, James V.; Carr, Brian S.; Baron, Richard L. (2000). «Extrahepatic Metastases of Hepatocellular Carcinoma». Radiology. 216 (3): 698–703. doi:10.1148/radiology.216.3.r00se24698. PMID 10966697.
- ↑ «Hepatitis B: Prevention and treatment». Արխիվացված է օրիգինալից 24 July 2013-ին. Վերցված է 28 August 2013-ին. "WHO aims at controlling HBV worldwide to decrease the incidence of HBV-related chronic liver disease, cirrhosis, and hepatocellular carcinoma. by integrating HB vaccination into routine infant (and possibly adolescent) immunization programs."
- ↑ «Prevention». Վերցված է May 12, 2010-ին.
- ↑ 50,0 50,1 Pompili, Maurizio (2013). «Bridging and downstaging treatments for hepatocellular carcinoma in patients on the waiting list for liver transplantation». World Journal of Gastroenterology. 19 (43): 7515–30. doi:10.3748/wjg.v19.i43.7515. PMC 3837250. PMID 24282343.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Gbolahan, Olumide B.; Schacht, Michael A.; Beckley, Eric W.; LaRoche, Thomas P.; O'Neil, Bert H.; Pyko, Maximilian (April 2017). «Locoregional and systemic therapy for hepatocellular carcinoma». Journal of Gastrointestinal Oncology. 8 (2): 215–228. doi:10.21037/jgo.2017.03.13. ISSN 2078-6891. PMC 5401862. PMID 28480062.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Marrero, JA; Kulik, LM; Sirlin, CB; Zhu, AX; Finn, RS; Abecassis, MM; Roberts, LR; Heimbach, JK (August 2018). «Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases» (PDF). Hepatology. 68 (2): 723–750. doi:10.1002/hep.29913. PMID 29624699. S2CID 4666537.
- ↑ Ma, Ka Wing; Cheung, Tan To (December 2016). «Surgical resection of localized hepatocellular carcinoma: patient selection and special consideration». Journal of Hepatocellular Carcinoma. 4: 1–9. doi:10.2147/JHC.S96085. PMC 5207474. PMID 28097107.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Ang, Soo Fan; Ng, Elizabeth Shu-Hui; Li, Huihua; Ong, Yu-Han; Choo, Su Pin; Ngeow, Joanne; Toh, Han Chong; Lim, Kiat Hon; Yap, Hao Yun; Tan, Chee Kiat; Ooi, London Lucien Peng Jin; Chung, Alexander Yaw Fui; Chow, Pierce Kah Hoe; Foo, Kian Fong; Tan, Min-Han; Cheow, Peng Chung (2015). «The Singapore Liver Cancer Recurrence (SLICER) Score for Relapse Prediction in Patients with Surgically Resected Hepatocellular Carcinoma». PLOS ONE. 10 (4): e0118658. Bibcode:2015PLoSO..1018658A. doi:10.1371/journal.pone.0118658. PMC 4382157. PMID 25830231.
- ↑ Vitale, Alessandro; Gringeri, Enrico; Valmasoni, Michele; D'Amico, Francesco; Carraro, Amedeo; Pauletto, Alberto; D'Amico, Francesco Jr.; Polacco, Marina; D'Amico, Davide Francesco; Cillo, Umberto (2007). «Longterm results of liver transplantation for hepatocellular carcinoma: an update of the University of Padova experience». Transplantation Proceedings. 39 (6): 1892–1894. doi:10.1016/j.transproceed.2007.05.031. PMID 17692645.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Cillo, Umberto; Vitale, Alessandro; Bassanello, Marco; Boccagni, Patrizia; Brolese, Alberto; Zanus, Giacomo; Burra, Patrizia; Fagiuoli, Stefano; Farinati, Fabio; Rugge, Massimo; d'Amico, Davide Francesco (February 2004). «Liver transplantation for the treatment of moderately or well-differentiated hepatocellular carcinoma». Annals of Surgery. 239 (2): 150–9. doi:10.1097/01.sla.0000109146.72827.76. PMC 1356206. PMID 14745321.
- ↑ Tanabe, KK; Curley, SA; Dodd, GD; Siperstein, AE; Goldberg, SN (February 1, 2004). «Radiofrequency ablation: the experts weigh in». Cancer. 100 (3): 641–50. doi:10.1002/cncr.11919. PMID 14745883.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Tateishi, R; Shiina, S; Teratani, T; Obi, S; Sato, S; Koike, Y; Fujishima, T; Yoshida, H; Kawabe, T; Omata, M (15 March 2005). «Percutaneous radiofrequency ablation for hepatocellular carcinoma. An analysis of 1000 cases». Cancer. 103 (6): 1201–9. doi:10.1002/cncr.20892. PMID 15690326. S2CID 37178385.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Chen, Min-Shan; Li, Jin-Qing; Zheng, Yun; Guo, Rong-Ping; Liang, Hui-Hong; Zhang, Ya-Qi; Lin, Xiao-Jun; Lau, Wan Y (2006). «A Prospective Randomized Trial Comparing Percutaneous Local Ablative Therapy and Partial Hepatectomy for Small Hepatocellular Carcinoma». Annals of Surgery. 243 (3): 321–8. doi:10.1097/01.sla.0000201480.65519.b8. PMC 1448947. PMID 16495695.
- ↑ Yamamoto, Junji; Okada, Shuichi; Shimada, Kazuaki; Okusaka, Takushi; Yamasaki, Susumu; Ueno, Hideki; Kosuge, Tomoo (2001). «Treatment strategy for small hepatocellular carcinoma: Comparison of long-term results after percutaneous ethanol injection therapy and surgical resection». Hepatology. 34 (4): 707–713. doi:10.1053/jhep.2001.27950. PMID 11584366.
- ↑ «Interventional Radiology Treatments for Liver Cancer». Society of Interventional Radiology. Արխիվացված է օրիգինալից 8 February 2014-ին. Վերցված է 4 February 2014-ին.
- ↑ Kooby, DA; Egnatashvili, V; Srinivasan, S; Chamsuddin, A; Delman, KA; Kauh, J; Staley CA, 3rd; Kim, HS (February 2010). «Comparison of yttrium-90 radioembolization and transcatheter arterial chemoembolization for the treatment of unresectable hepatocellular carcinoma». Journal of Vascular and Interventional Radiology. 21 (2): 224–30. doi:10.1016/j.jvir.2009.10.013. PMID 20022765.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) CS1 սպաս․ թվային անուններ: authors list (link) - ↑ «Hepatocellular Carcinoma (HCC) and Liver Metastases». The Lecturio Medical Concept Library. Վերցված է 4 July 2021-ին.
- ↑ Jonathan Klein (2012). «Hepatocellular Carcinoma Radiation Therapy: Review of Evidence and Future Opportunities». Nt J Radiation Oncol Biol Phys. 87 (1): 22–32. doi:10.1016/j.ijrobp.2012.08.043. PMID 23219567.
- ↑ Mutlay Sayan (2019). «Rethinking the Role of Radiation Therapy in the Treatment of Unresectable Hepatocellular Carcinoma: A Data Driven Treatment Algorithm for Optimizing Outcomes». Front. Oncol. 9: 345. doi:10.3389/fonc.2019.00345. PMC 6591511. PMID 31275846.
- ↑ Nina N Sanford (2018). «Protons versus Photons for Unresectable Hepatocellular Carcinoma: Liver Decompensation and Overall Survival». Int J Radiation Oncol Biol Phys. 105 (1): 64–72. doi:10.1016/j.ijrobp.2019.01.076. PMID 30684667.
- ↑ «Radiation Therapy With Protons or Photons in Treating Patients With Liver Cancer». ClinicalTrials.gov. 21 Aug 2020.
- ↑ Lin, Shi-Ming (21 Aug 2020). «Proton Radiotherapy Versus Radiofrequency Ablation for Patients With Medium or Large Hepatocellular Carcinoma». ClinicalTrials.gov.
- ↑ Md, Michael Devera (21 Aug 2020). «Transarterial Chemoembolization Versus Proton Beam Radiotherapy for the Treatment of Hepatocellular Carcinoma». ClinicalTrials.gov.
- ↑ 70,0 70,1 Llovet, Josep M.; Ricci, Sergio; Mazzaferro, Vincenzo; Hilgard, Philip; Gane, Edward; Blanc, Jean-Frédéric; de Oliveira, Andre Cosme; Santoro, Armando; Raoul, Jean-Luc (2008-07-24). «Sorafenib in Advanced Hepatocellular Carcinoma». New England Journal of Medicine. 359 (4): 378–390. CiteSeerX 10.1.1.531.1130. doi:10.1056/nejmoa0708857. ISSN 0028-4793. PMID 18650514.
- ↑ 71,0 71,1 Cheng, Ann-Lii; Kang, Yoon-Koo; Chen, Zhendong; Tsao, Chao-Jung; Qin, Shukui; Kim, Jun Suk; Luo, Rongcheng; Feng, Jifeng; Ye, Shenglong (January 2009). «Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial». The Lancet. Oncology. 10 (1): 25–34. doi:10.1016/S1470-2045(08)70285-7. ISSN 1474-5488. PMID 19095497.
- ↑ Kudo, Masatoshi (2017). «Systemic Therapy for Hepatocellular Carcinoma: 2017 Update». Oncology (անգլերեն). 93 (1): 135–146. doi:10.1159/000481244. ISSN 0030-2414. PMID 29258077.
- ↑ Finn, Richard S.; Qin, Shukui; Ikeda, Masafumi; Galle, Peter R.; Ducreux, Michel; Kim, Tae-You; Kudo, Masatoshi; Breder, Valeriy; Merle, Philippe; Kaseb, Ahmed O.; Li, Daneng; Verret, Wendy; Xu, Derek-Zhen; Hernandez, Sairy; Liu, Juan; Huang, Chen; Mulla, Sohail; Wang, Yulei; Lim, Ho Yeong; Zhu, Andrew X.; Cheng, Ann-Lii (2020). «Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma». New England Journal of Medicine. 382 (20): 1894–1905. doi:10.1056/nejmoa1915745. PMID 32402160. S2CID 218633632.
- ↑ 74,0 74,1 «Imjudo (tremelimumab) in combination with Imfinzi approved in the US for patients with unresectable liver cancer». AstraZeneca (Press release). 26 October 2022. Վերցված է 26 October 2022-ին.
- ↑ Madoff, DC; Hicks, ME; Vauthey, JN; Charnsangavej, C; Morello FA, Jr; Ahrar, K; Wallace, MJ; Gupta, S (September–October 2002). «Transhepatic portal vein embolization: anatomy, indications, and technical considerations». Radiographics. 22 (5): 1063–76. doi:10.1148/radiographics.22.5.g02se161063. PMID 12235336.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Vente MA, Wondergem M, van der Tweel I, և այլք: (April 2009). «Yttrium-90 microsphere radioembolization for the treatment of liver malignancies: a structured meta-analysis». European Radiology. 19 (4): 951–9. doi:10.1007/s00330-008-1211-7. PMID 18989675.
- ↑ Hepatocellular carcinoma Արխիվացված 2016-07-05 Wayback Machine MedlinePlus, Medical Encyclopedia
- ↑ «WHO Disease and injury country estimates». World Health Organization. 2009. Վերցված է November 11, 2009-ին.
- ↑ Table 37.2 Արխիվացված 2020-02-24 Wayback Machine in: Sternberg, Stephen (2012). Sternberg's diagnostic surgical pathology. Place of publication not identified: LWW. ISBN 978-1-4511-5289-0. OCLC 953861627.
- ↑ 80,0 80,1 Kumar V, Fausto N, Abbas A (editors) (2015). Robbins & Cotran Pathologic Basis of Disease (9th ed.). Elsevier/Saunders. էջեր 821–881. ISBN 9780323266161.
{{cite book}}:|author=has generic name (օգնություն)CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ «Cancer». World Health Organization. February 2006. Վերցված է 2007-05-24-ին.
- ↑ Rowe, JulieH; Ghouri, YezazAhmed; Mian, Idrees (2017-01-01). «Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis». Journal of Carcinogenesis (անգլերեն). 16 (1): 1. doi:10.4103/jcar.jcar_9_16. PMC 5490340. PMID 28694740.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Choo, Su Pin; Tan, Wan Ling; Goh, Brian K. P.; Tai, Wai Meng; Zhu, Andrew X. (15 November 2016). «Comparison of hepatocellular carcinoma in Eastern versus Western populations». Cancer. 122 (22): 3430–3446. doi:10.1002/cncr.30237. PMID 27622302. S2CID 42804844.
- ↑ Goh, George Boon-Bee; Chang, Pik-Eu; Tan, Chee-Kiat (December 2015). «Changing epidemiology of hepatocellular carcinoma in Asia». Best Practice & Research Clinical Gastroenterology. 29 (6): 919–928. doi:10.1016/j.bpg.2015.09.007. PMID 26651253.
- ↑ phyton (2016-08-22). «Phyton Biotech Achieves Manufacturing Milestone with Thapsigargin, the Active Agent in Mipsagargin». Phyton Biotech (ամերիկյան անգլերեն). Վերցված է 2020-04-10-ին.
- ↑ Mahalingam, Devalingam; Peguero, Julio; Cen, Putao; Arora, Sukeshi P.; Sarantopoulos, John; Rowe, Julie; Allgood, Victoria; Tubb, Benjamin; Campos, Luis (2019-06-17). «A Phase II, Multicenter, Single-Arm Study of Mipsagargin (G-202) as a Second-Line Therapy Following Sorafenib for Adult Patients with Progressive Advanced Hepatocellular Carcinoma». Cancers. 11 (6): 833. doi:10.3390/cancers11060833. ISSN 2072-6694. PMC 6627768. PMID 31212948.
- ↑ Yang, Jian-min; Wang, Hui-ju; Du, Ling; Han, Xiao-mei; Ye, Zai-yuan; Fang, Yong; Tao, Hou-quan; Zhao, Zhong-sheng; Zhou, Yong-lie (2009-01-25). «Screening and identification of novel B cell epitopes in human heparanase and their anti-invasion property for hepatocellular carcinoma». Cancer Immunology, Immunotherapy. 58 (9): 1387–1396. doi:10.1007/s00262-008-0651-x. PMID 19169879. S2CID 19074169.
- ↑ «Huntington Medical Research Institute News, May 2005» (PDF). Արխիվացված է օրիգինալից (PDF) December 10, 2005-ին.
- ↑ Klingenberg, Marcel; Matsuda, Akiko; Diederichs, Sven; Patel, Tushar (September 2017). «Non-coding RNA in hepatocellular carcinoma: Mechanisms, biomarkers and therapeutic targets». Journal of Hepatology. 67 (3): 603–618. doi:10.1016/j.jhep.2017.04.009. ISSN 1600-0641. PMID 28438689.
- ↑ Braconi, C; Valeri, N, Kogure, T, Gasparini, P, Huang, N, Nuovo, GJ, Terracciano, L, Croce, CM, Patel, T (2011-01-11). «Expression and functional role of a transcribed noncoding RNA with an ultraconserved element in hepatocellular carcinoma». Proceedings of the National Academy of Sciences of the United States of America. 108 (2): 786–91. Bibcode:2011PNAS..108..786B. doi:10.1073/pnas.1011098108. PMC 3021052. PMID 21187392.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ «Journal of Clinical Oncology, Special Issue on Molecular Oncology: Receptor-Based Therapy, April 2005». Արխիվացված է օրիգինալից 2005-11-30-ին. Վերցված է 2005-08-31-ին.
- ↑ Lau W, Leung T, Ho S, Chan M, Machin D, Lau J, Chan A, Yeo W, Mok T, Yu S, Leung N, Johnson P (1999). «Adjuvant intra-arterial iodine-131-labelled lipiodol for resectable hepatocellular carcinoma: a prospective randomised trial». The Lancet. 353 (9155): 797–801. doi:10.1016/S0140-6736(98)06475-7. PMID 10459961. S2CID 54270315.
- ↑ Thomas M, Zhu A (2005). «Hepatocellular carcinoma: the need for progress». Journal of Clinical Oncology. 23 (13): 2892–9. doi:10.1200/JCO.2005.03.196. PMID 15860847. Արխիվացված է օրիգինալից 2005-11-05-ին. Վերցված է 2005-08-29-ին.
- ↑ Broutier L, Mastrogiovanni G, Verstegen MM, Francies HE, Gavarró LM, Bradshaw CR, Allen GE, Arnes-Benito R, Sidorova O, Gaspersz MP, Georgakopoulos N, Koo BK, Dietmann S, Davies SE, Praseedom RK, Lieshout R, IJzermans JNM, Wigmore SJ, Saeb-Parsy K, Garnett MJ, van der Laan LJ, Huch M (2017). «Human primary liver cancer-derived organoid cultures for disease modeling and drug screening». Nat Med. 23 (12): 1424–1435. doi:10.1038/nm.4438. PMC 5722201. PMID 29131160.
{{cite journal}}: CS1 սպաս․ բազմաթիվ անուններ: authors list (link) - ↑ Fumao, B; Zhou, H; Ma, M; Guan, C; Lyu, J; Meng, QH (2 May 2018). «A novel RNA-sequencing-based miRNA signature predicts with recurrence and outcome of hepatocellular carcinoma». Molecular Oncology. 12 (7): 1125–1137. doi:10.1002/1878-0261.12315. PMC 6026871. PMID 29719937.
- ↑ «ennerex Granted FDA Orphan Drug Designation for Pexa-Vec in Hepatocellular Carcinoma (HCC)». Արխիվացված է օրիգինալից March 25, 2014-ին.
- ↑ «Enforcement Reports». www.accessdata.fda.gov.
- ↑ Tarakanovskaya, M. G; Chinburen, J; Batchuluun, P; Munkhzaya, C; Purevsuren, G; Dandii, D; Hulan, T; Oyungerel, D; Kutsyna, G. A; Reid, A. A; Borisova, V; Bain, A. I; Jirathitikal, V; Bourinbaiar, A. S (2017). «Open-label Phase II clinical trial in 75 patients with advanced hepatocellular carcinoma receiving daily dose of tableted liver cancer vaccine, hepcortespenlisimut-L». Journal of Hepatocellular Carcinoma. 4: 59–69. doi:10.2147/JHC.S122507. PMC 5396941. PMID 28443252.
{{cite journal}}: CS1 սպաս․ չպիտակված ազատ DOI (link) - ↑ Sanoff, Hanna K.; Kim, Richard; Ivanova, Anastasia; Alistar, Angela; McRee, Autumn J.; O’Neil, Bert H. (2015). «Everolimus and pasireotide for advanced and metastatic hepatocellular carcinoma». Investigational New Drugs. 33 (2): 505–509. doi:10.1007/s10637-015-0209-7. PMC 4487887. PMID 25613083.
Further reading[խմբագրել | խմբագրել կոդը]
- «Long-term results of liver transplantation for hepatocellular carcinoma: an update of the University of Padova experience». September 23, 2013. Վերցված է 6 February 2014-ին.
- Bruix, Jordi; Sherman, Morris; Practice Guidelines Committee (November 2005). «Management of hepatocellular carcinoma». Hepatology. 42 (5): 1208–1236. doi:10.1002/hep.20933. PMID 16250051. S2CID 5106445.
- Liu, Chi-leung, M.D., "Hepatic Resection for Hepatocellular Carcinoma" Արխիվացված 2021-04-15 Wayback Machine, The Hong Kong Medical Diary, Vol.10 No.12, December 2005 Medical Bulletin