
Մասնակից:Mariamus Medicus/Ավազարկղ2
Ախտորոշում[խմբագրել | խմբագրել կոդը]

ԹՔՕՀ ախտորոշումը պռտք է դիտարկվի յուրաքանչյուր 30-45 տարեկանից բարձր դժվարաշնչություն, քրոնիկ հազ և խորխորտադրություն ունեցող մարդու մոտ, կամ նրա մոտ, ով հաճախակի ունենում է սեզոնային մրսածության նշաններ կամ ենթարկվում է հիվանդության ռիսկի գործոնի ազդեցությանը[1][2]: Այնուհետև ատտորոշման հաստատման նպատակով կիրառվում է սպիրոմետրիան[1][3]: Ախտանշանների բացակայության դեպքում ախտորոշիչ մեթոդի սկրինինգ անցկացումը խորհուրդ չի տրվում[4]:
Spirometry[խմբագրել | խմբագրել կոդը]
Spirometry measures the amount of airflow obstruction present and is generally carried out after the use of a bronchodilator, a medication to open up the airways.[3] Two main components are measured to make the diagnosis, the forced expiratory volume in one second (FEV1), which is the greatest volume of air that can be breathed out in the first second of a breath, and the forced vital capacity (FVC), which is the greatest volume of air that can be breathed out in a single large breath.[5] Normally, 75–80% of the FVC comes out in the first second[5] and a FEV1/FVC ratio less than 70% in someone with symptoms of COPD defines a person as having the disease.[3] Based on these measurements, spirometry would lead to over-diagnosis of COPD in the elderly.[3] The National Institute for Health and Care Excellence criteria additionally require a FEV1 less than 80% of predicted.[2] People with COPD also exhibit a decrease in diffusing capacity of the lung for carbon monoxide (DLCO) due to decreased surface area in the alveoli, as well as damage to the capillary bed.[6]
Evidence for using spirometry among those without symptoms in an effort to diagnose the condition earlier is of uncertain effect, so currently is not recommended.[1][3] A peak expiratory flow (the maximum speed of expiration), commonly used in asthma, is not sufficient for the diagnosis of COPD.[2]
Severity[խմբագրել | խմբագրել կոդը]
| Grade | Activity affected |
|---|---|
| 1 | Only strenuous activity |
| 2 | Vigorous walking |
| 3 | With normal walking |
| 4 | After a few minutes of walking |
| 5 | With changing clothing |
| Severity | FEV1 % predicted |
|---|---|
| Mild (GOLD 1) | ≥80 |
| Moderate (GOLD 2) | 50–79 |
| Severe (GOLD 3) | 30–49 |
| Very severe (GOLD 4) | <30 |
A number of methods can determine how much COPD is affecting a given individual.[1] The modified British Medical Research Council questionnaire or the COPD assessment test (CAT) are simple questionnaires that may be used to determine the severity of symptoms.[1] Scores on CAT range from 0–40 with the higher the score, the more severe the disease.[7] Spirometry may help to determine the severity of airflow limitation.[1] This is typically based on the FEV1 expressed as a percentage of the predicted "normal" for the person's age, gender, height, and weight.[1] Both the American and European guidelines recommended partly basing treatment recommendations on the FEV1.[3] The GOLD guidelines suggest dividing people into four categories based on symptoms assessment and airflow limitation.[1] Weight loss and muscle weakness, as well as the presence of other diseases, should also be taken into account.[1]
Other tests[խմբագրել | խմբագրել կոդը]
A chest X-ray and complete blood count may be useful to exclude other conditions at the time of diagnosis.[8] Characteristic signs on X-ray are overexpanded lungs, a flattened diaphragm, increased retrosternal airspace, and bullae, while it can help exclude other lung diseases, such as pneumonia, pulmonary edema, or a pneumothorax.[9] A high-resolution computed tomography scan of the chest may show the distribution of emphysema throughout the lungs and can also be useful to exclude other lung diseases.[10] Unless surgery is planned, however, this rarely affects management.[10] An analysis of arterial blood is used to determine the need for oxygen; this is recommended in those with an FEV1 less than 35% predicted, those with a peripheral oxygen saturation less than 92%, and those with symptoms of congestive heart failure.[1] In areas of the world where alpha-1 antitrypsin deficiency is common, people with COPD (particularly those below the age of 45 and with emphysema affecting the lower parts of the lungs) should be considered for testing.[1]
-
 Chest X-ray demonstrating severe COPD: Note the small heart size in comparison to the lungs.
Chest X-ray demonstrating severe COPD: Note the small heart size in comparison to the lungs. -
 A lateral chest X-ray of a person with emphysema: Note the barrel chest and flat diaphragm.
A lateral chest X-ray of a person with emphysema: Note the barrel chest and flat diaphragm. -
 Lung bulla as seen on chest X-ray in a person with severe COPD
Lung bulla as seen on chest X-ray in a person with severe COPD -
 A severe case of bullous emphysema
A severe case of bullous emphysema -
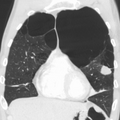
 Axial CT image of the lung of a person with end-stage bullous emphysema
Axial CT image of the lung of a person with end-stage bullous emphysema -
 Very severe emphysema with lung cancer on the left (CT scan)
Very severe emphysema with lung cancer on the left (CT scan)






- ↑ 1,00 1,01 1,02 1,03 1,04 1,05 1,06 1,07 1,08 1,09 1,10 1,11 Քաղվածելու սխալ՝ Սխալ
<ref>պիտակ՝ «GOLD2013Chp2» անվանումով ref-երը տեքստ չեն պարունակում: - ↑ 2,0 2,1 2,2 2,3 Քաղվածելու սխալ՝ Սխալ
<ref>պիտակ՝ «NICE2010P60» անվանումով ref-երը տեքստ չեն պարունակում: - ↑ 3,0 3,1 3,2 3,3 3,4 3,5 Qaseem, Amir; Wilt, TJ; Weinberger, SE; Hanania, NA; Criner, G; Van Der Molen, T; Marciniuk, DD; Denberg, T; Schünemann, H; Wedzicha, W; MacDonald, R; Shekelle, P; American College Of Physicians; American College of Chest Physicians; American Thoracic Society; European Respiratory Society (2011). «Diagnosis and Management of Stable Chronic Obstructive Pulmonary Disease: A Clinical Practice Guideline Update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society». Annals of Internal Medicine. 155 (3): 179–91. doi:10.7326/0003-4819-155-3-201108020-00008. PMID 21810710. Արխիվացված է օրիգինալից 2014-10-12-ին.
{{cite journal}}: Unknown parameter|deadurl=ignored (|url-status=suggested) (օգնություն) - ↑ Siu, Albert L.; Bibbins-Domingo, Kirsten; Grossman, David C.; Davidson, Karina W.; Epling, John W.; García, Francisco A. R.; Gillman, Matthew; Kemper, Alex R.; Krist, Alex H.; Kurth, Ann E.; Landefeld, C. Seth; Mangione, Carol M.; Harper, Diane M.; Phillips, William R.; Phipps, Maureen G.; Pignone, Michael P. (5 April 2016). «Screening for Chronic Obstructive Pulmonary Disease». JAMA. 315 (13): 1372. doi:10.1001/jama.2016.2638.
- ↑ 5,0 5,1 Young, Vincent B. (2010). Blueprints medicine (5th ed.). Wolters Kluwer Health/Lippincott Williams & Wilkins. էջ 69. ISBN 978-0-7817-8870-0. Արխիվացված է օրիգինալից 2016-05-17-ին.
{{cite book}}: Unknown parameter|deadurl=ignored (|url-status=suggested) (օգնություն) - ↑ Bailey, Kristina L. (1 July 2012). «The Importance of the Assessment of Pulmonary Function in COPD». The Medical clinics of North America. 96 (4): 745–752. doi:10.1016/j.mcna.2012.04.011. ISSN 0025-7125. PMC 3998207. PMID 22793942.
- ↑ «COPD Assessment Test (CAT)». American Thoracic Society. Արխիվացված է օրիգինալից December 3, 2013-ին. Վերցված է November 29, 2013-ին.
{{cite web}}: Unknown parameter|deadurl=ignored (|url-status=suggested) (օգնություն) - ↑ Քաղվածելու սխալ՝ Սխալ
<ref>պիտակ՝ «NICE2010P70» անվանումով ref-երը տեքստ չեն պարունակում: - ↑ Torres M, Moayedi S (May 2007). «Evaluation of the acutely dyspneic elderly patient». Clin. Geriatr. Med. 23 (2): 307–25, vi. doi:10.1016/j.cger.2007.01.007. PMID 17462519.
- ↑ 10,0 10,1 Քաղվածելու սխալ՝ Սխալ
<ref>պիտակ՝ «Harr2012» անվանումով ref-երը տեքստ չեն պարունակում: